
Case 13: Special Report 13 — Orthodontic Extrusion Prior to the Placement of Adjacent Implants for a More Esthetically Pleasing Smile
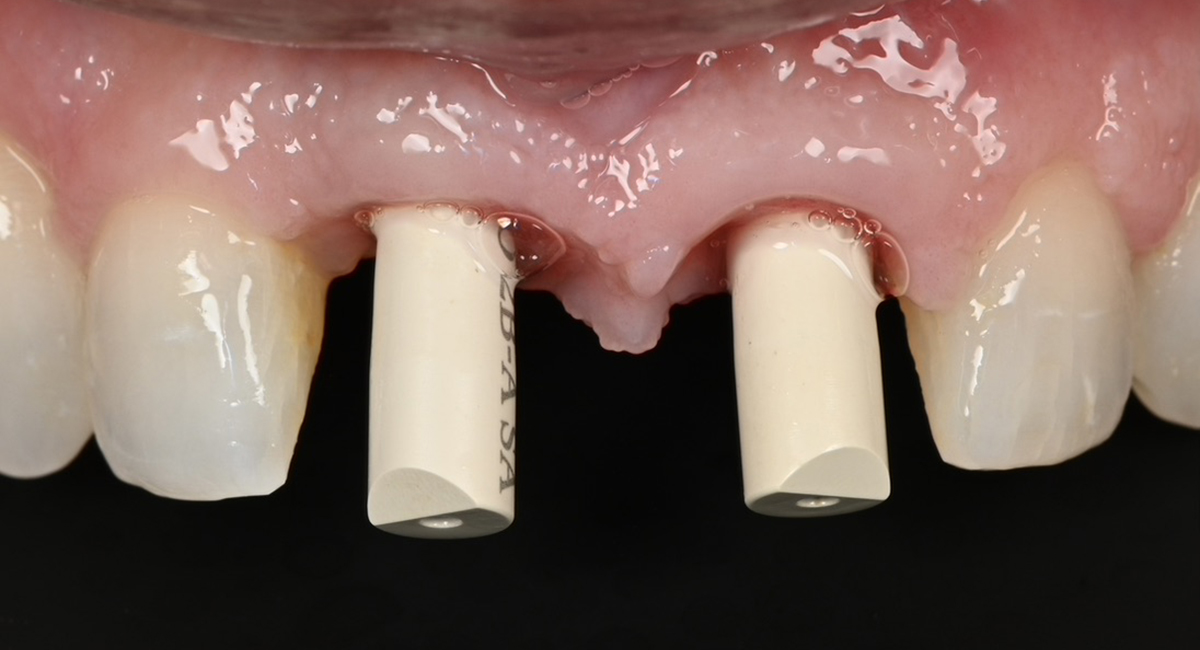
Implant restoration in the esthetic zone often requires well-coordinated interdisciplinary care in order to achieve ideal treatment results. This is especially the case when implants are planned to replace periodontally hopeless teeth. When teeth are extracted, we can typically anticipate 2mm of facial recession. If implants are to be placed following the extraction of hopeless teeth with an already existing gingival height discrepancy, the discrepancy will likely be exacerbated.
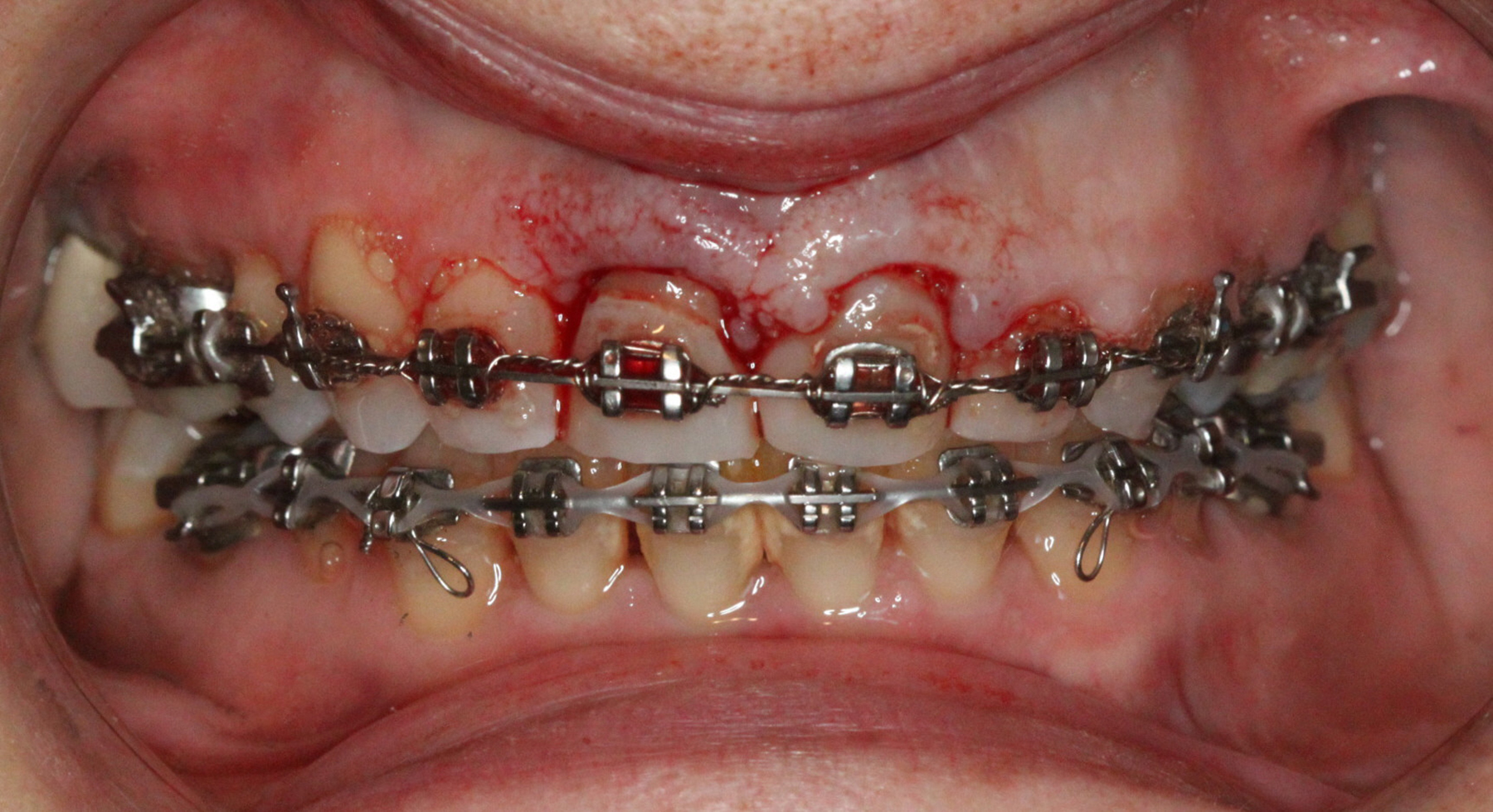
Extraction after forced eruption can allow for a much more favorable implant site compared with extraction alone. This is possible because the tension applied to the periodontal ligament during orthodontic tooth movement stimulates osteoblastic activity to induce new bone formation. As the tooth moves coronally during extrusion, soft tissue and bone attached to the periodontal fibers migrate in the same direction. As a result, forced eruption can be used to enhance the quality and quantity of both hard and soft tissue of future implant sites.
The special report presented below illustrates how orthodontic extrusion was successfully used to improve the periodontal architecture prior to the placement of two adjacent implants in the esthetic zone and thus allowed for a more ideal restorative result.