Air abrasion, or sandblasting, is a procedure very commonly used in the dental laboratory to clean restorations or give them surface texture prior to bonding. Intraoral air abrasion is using the same technique to clean and smooth tooth preparations in the mouth prior to bonding. It can be used for cleaning direct composite preparations, indirect crown, or onlay preparations. This article will present instrumentation used for intraoral abrasion, the science behind the technique, and some clinical tips for performing this procedure.
Instrumentation
In order to perform this technique, the armamentarium includes an air abrasion device and abrasive particles. Air abrasion devices can be classified into those used with simultaneous application of water and those used without water. An example of a device used without water is the Microetcher II (Danville). This device connects to the air lines commonly found on dental units. The advantage of this device is that it is portable and relatively inexpensive. It can be used for intraoral abrasion and transferred to a dental laboratory space to clean restorations extra-orally. A cannister in the back of the device holds the abrasive particles. Different cannisters can be stored with different types of abrasive particles.

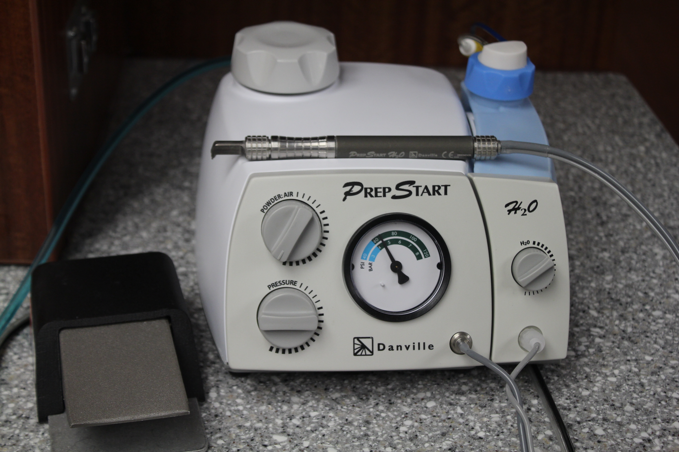
Other abrasion devices simultaneously apply abrasive particles and water. The purpose of the water is to control the spray of abrasive particles. Practically it helps to prevent the particles from coating the patients mouth and travelling through the air onto the patient, the operator and the assistant. In the author’s opinion, a device with simultaneous water application improves the operator experience if air abrasion is part of a daily bonding routine. An example of a device used with simultaneous water application is the PrepStart H2O. This device also connects to an air line. Water is supplied from a built-in cannister that can be refilled by hand with the same water used in the dental unit. The abrasive particles are added to a separate built-in canister that can be filled with any type of abrasive particles. This device allows the operator to adjust the amount of particle spray, water spray and the air pressure. The device is operated by a foot pedal.
The abrasive particle most commonly used for intraoral abrasion prior to bonding is 50 micron alumina. Alumina is the most abrasive type of particle used in dentistry due to its density and sharp edges. This is also the type of particle used for cleaning zirconia restorations. Softer abrasive particles, such as sodium bicarbonate or glycine, have been used for dental cleanings (air polishing) because they remove plaque without affecting the underlying tooth structure. Another softer particle, aluminum trihydroxide, is used with intraoral abrasion to remove biofilm prior to bonding. Glass beads are another type of abrasive particle used in the dental laboratory. Glass beads are less abrasive than alumina and can be used to clean off temporary or permanent cement. The author uses 50 micron alumina in a PrepStart H2O for cleaning teeth and zirconia, and separate cannisters of 50 micron alumina and glass beads in the Microetcher II for cleaning cement.
The Science
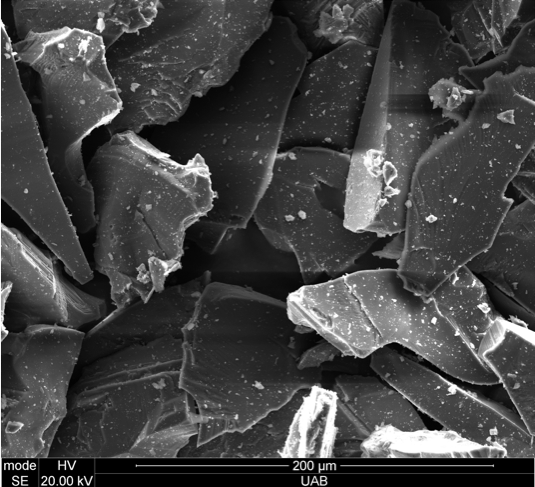
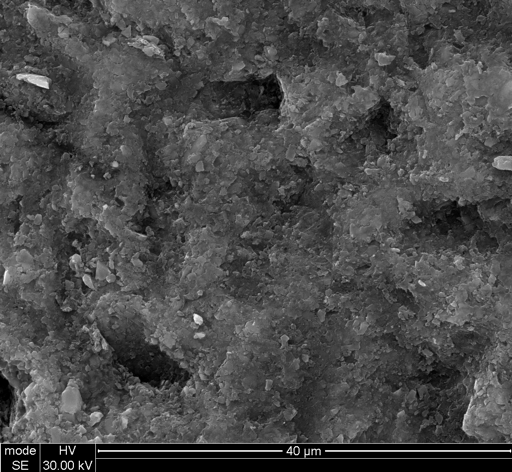
Intraoral abrasion will produce surface texture on enamel, dentin and composite. The texture produced on enamel and dentin is slightly coarser than the acid etch pattern of enamel or that of exposed dentinal tubules. Several researchers (including the author) have evaluated the effect of intraoral abrasion on the bond to enamel and dentin using laboratory studies. In general, the bond to enamel and dentin is not significantly affected by air abrasion.1-6 These results may seem to contradict the proposed benefits of air abrasion of preparations prior to bonding. However, laboratory studies measure the bond to clean tooth surfaces. In the author’s opinion, the purpose of intraoral abrasion is to clean the tooth surface of any contaminants (old restorative material, staining, unsupported enamel, etc.) prior to bonding.


Intraoral abrasion will also place surface texture on composite or build-up materials that may be present on a tooth preparation. The texture produced from air abrasion will improve the bond to an aged composite-based material.7,8
Clinical Tips
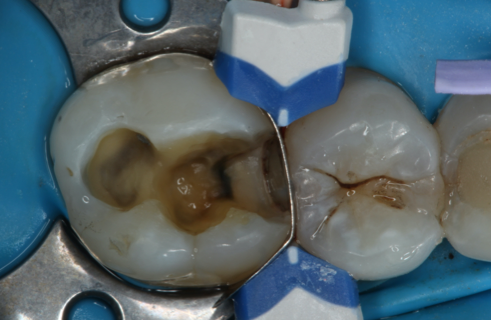
Intraoral abrasion will give tooth preparations a smooth, dull and clean appearance. It can help to remove any old restorative material, staining, hemostatic agent, temporary cement, unsupported enamel, and irregularities in the preparation. Air abrasion can remove carious dentin, however, it was shown that it does not remove it selectively.9,10 In other words, air abrasion will not differentiate between non-carious and carious dentin.

Even though simultaneous water application helps to control the particle spray, the air particles need to be removed for patient comfort. Rubber dam and Iso-vac isolation works well to prevent particles from collecting in the patient’s mouth. Alternatively, gauze and a high-volume evacuator can help prevent most particles from settling in the patient’s mouth.
In the author’s experience, air abrasion does not produce any sensitivity beyond what is produced from air/water spray. In many cases, the author has used air abrasion to clean a tooth surface without the use of local anesthetic prior to bonding an indirect restoration, bonding a direct composite to enamel, or repairing an old composite restoration. Air abrasion should be directed to avoid soft tissue. Although air abrasion on soft tissue does not typically produce pain or tissue damage, it may create bleeding that will interfere with bonding.
Air abrasion with alumina particles has been shown to create surface texture on zirconia and clean salivary contamination from zirconia crowns prior to bonding.11 A study by the author has demonstrated that abrasion of zirconia with the intraoral device (PrepStart H2O) was as effective at creating bonding texture as using a laboratory sandblaster.1 The author will often use the intraoral abrasion device to clean both the tooth preparation and the zirconia crown prior to bonding the crown. Air abrasion of glass ceramics with alumina abrasive particles, however, is not recommended as it will decrease its strength.12 Any cleaning of glass ceramics should be performed with glass beads.
Summary
Intraoral air abrasion is a technique that will clean tooth structure and build-up material prior to direct or indirect bonding. A device without simultaneous water, such as the Microetcher II, may be a first step into using this technique due to its lower cost. If this technique becomes part of a regular bonding protocol, a device with simultaneous water spray will make the process easier for both the operator and the patient.
Shop Zest Dental Solutions
References
- Huang CT, Kim J, Arce C, Lawson NC. Intraoral Air Abrasion: A Review of Devices, Materials, Evidence, and Clinical Applications in Restorative Dentistry. Compend Contin Educ Dent. 2019 Sep;40(8):508-513; quiz 514.
- de Souza-Zaroni WC, Delfino CS, Ciccone-Nogueira JC, et al. Effect of cavity preparation method on microtensile bond strength of a self-etching primer vs phosphoric acid etchant to enamel. J Mater Sci Mater Med. 2007;18(10):2003-2009.
- Nikaido T, Kataumi M, Burrow MF, et al. Bond strengths of resin to enamel and dentin treated with low-pressure air abrasion. Oper Dent. 1996;21(5):218-224.
- Roeder LB, Berry EA 3rd, You C, Powers JM. Bond strength of composite to air-abraded enamel and dentin. Oper Dent. 1995;20(5):186-190.
- Los SA, Barkmeier WW. Effects of dentin air abrasion with aluminum oxide and hydroxyapatite on adhesive bond strength. Oper Dent. 1994;19(5):169-175.
- Van Meerbeek B, De Munck J, Mattar D, Van Landuyt K, Lambrechts P. Microtensile bond strengths of an etch&rinse and self-etch adhesive to enamel and dentin as a function of surface treatment. Oper Dent. 2003 Sep-Oct;28(5):647-60.
- Fornazari IA, Wille I, Meda EM, Brum RT, Souza EM. Effect of Surface Treatment, Silane, and Universal Adhesive on Microshear Bond Strength of Nanofilled Composite Repairs. Oper Dent. 2017 Jul/Aug;42(4):367-374.
- Baena E, Vignolo V, Fuentes MV, Ceballos L. Influence of repair procedure on composite-to-composite microtensile bond strength. Am J Dent. 2015 Oct;28(5):255-60.
- Paolinelis G, Watson TF, Banerjee A. Microhardness as a predictor of sound and carious dentine removal using alumina air abrasion. Caries Res. 2006;40(4):292-295.
- Motisuki C, Lima LM, Bronzi ES, et al. The effectiveness of alumina powder on carious dentin removal. Oper Dent. 2006;31(3):371-376
- Angkasith P, Burgess JO, Bottino MC, Lawson NC. Cleaning Methods for Zirconia Following Salivary Contamination. J Prosthodont. 2016 Jul;25(5):375-9.
- Menees TS, Lawson NC, Beck PR, Burgess JO. Influence of particle abrasion or hydrofluoric acid etching on lithium disilicate flexural strength J Prosthet Dent. 2014 Nov;112(5):1164-70.